The GOOD!
Sealants are a thin layer of plastic that are placed on newly erupted teeth in children in an attempt to prevent the most common decay in young children. Sealants are designed for easy application to fill in the cracks and pits on the biting surface of back teeth that have the highest chance of bacterial infection that cause cavities. When doing dental work on a young child, you need to place a sealant quickly, as they generally have a hard time sitting still for any dental work.
The biting surface of a tooth is not a smooth surface, it has pits and fissures, or bumps and valleys, on the biting surface. When a tooth is formed in a child there are 5 lobes of enamel that grow together. Different teeth have different formations of the lobes, but they all have 5. Think of 5 white balloons that are squeezed together. Where two balloons touch you will have a line, where three or four touch, you will have lines that connect and make a pit. Those pits and lines are very small, but they can be very deep, and bacteria can penetrate down into them where a toothbrush cannot reach.
The bacteria that get lodged in the pits and fissures eat food particles that also push into the pits and fissures. Their byproduct of digestion is acid that dissolves the minerals in the enamel, weakens the structure, and burrows a hole into the tooth. We call the hole formed by the bacterial acid decay a cavity. No matter how diligent a parent or child is in their oral care, the bacteria cannot be removed in deep pits and fissures and, in many children, decay on the biting surface will form.
Sealants are designed to fill the pits and fissures with a thin composite resin and prevent the bacteria from penetrating into the tooth. If bacteria are already in the pits and fissures, then the concept is that the sealant will entomb the bacteria and prevent them from causing decay.
Research shows that Cavities (also known as caries or tooth decay) are one of the most common chronic diseases of childhood in the United States. Untreated cavities can cause pain and infections that may lead to problems with eating, speaking, playing, and learning. Children who have poor oral health often miss more school and receive lower grades than children who don’t. Here are some facts from the CDC:
- More than half of children aged 6 to 8 have had a cavity in at least one of their baby (primary) teeth.1
- More than half of adolescents aged 12 to 19 have had a cavity in at least one of their permanent teeth.1
- Children aged 5 to 19 years from low-income families are twice as likely (25%) to have cavities, compared with children from higher-income households (11%).
Sealants, when placed in children, reduce childhood cavity rates dramatically. Dental sealants can also prevent cavities for many years. Applying dental sealants to the chewing surfaces of the back teeth prevents 80% of cavities in children.
The usual method for placing a sealant is to clean the tooth with pumice, acid etch the enamel with phosphoric acid gel, rinse the acid off, dry the tooth (and keep it dry), place the resin sealant, and light cure it. All of this is done as quickly as possible in a small mouth attached to a moving child who (in many cases) does not want the sealant. Even with all those steps and obstacles, sealants do very well, 80% of the time. The 20% failure in sealants happens when the sealant comes off or decay progresses under the sealant.
The BAD
While sealants are great, they are not perfect, and they can be technique sensitive. The sealing resin can only bond to clean and prepared enamel. If there is any bacteria or plaque on the tooth, then the resin will not bond, and the sealant will leak or fall off. The concept of entombing the bacteria does not always work and sometimes the decay progresses under a sealant. When the decay is seen, some patients will not want to treat it, believing that the tooth has had a sealant and cannot get decay.
Many people get frustrated when a sealant fails or needs to be replaced and therefore believe that they do not work at all. It is a struggle to explain to patients that using a personal experience as the sole determent of the success of a procedure is a sample size of one. As I always say, “The plural of anecdote is not data.” There are vastly more cavities prevented by sealants.
Even with the problems of traditional sealants, when you look at large sample sizes of kids and cavity rates, they do a great job at reducing pit and fissure cavities in children.
The IDEAL
The IDEAL placement technique for a sealant is debated among dentists. However, research has shown that the most successful long-term sealants are done in the following manner. This ideal sealant process is also called a Preventative Resin Restoration (PRR) and the steps mimic a filling. No numbing is required, but there is some drilling.
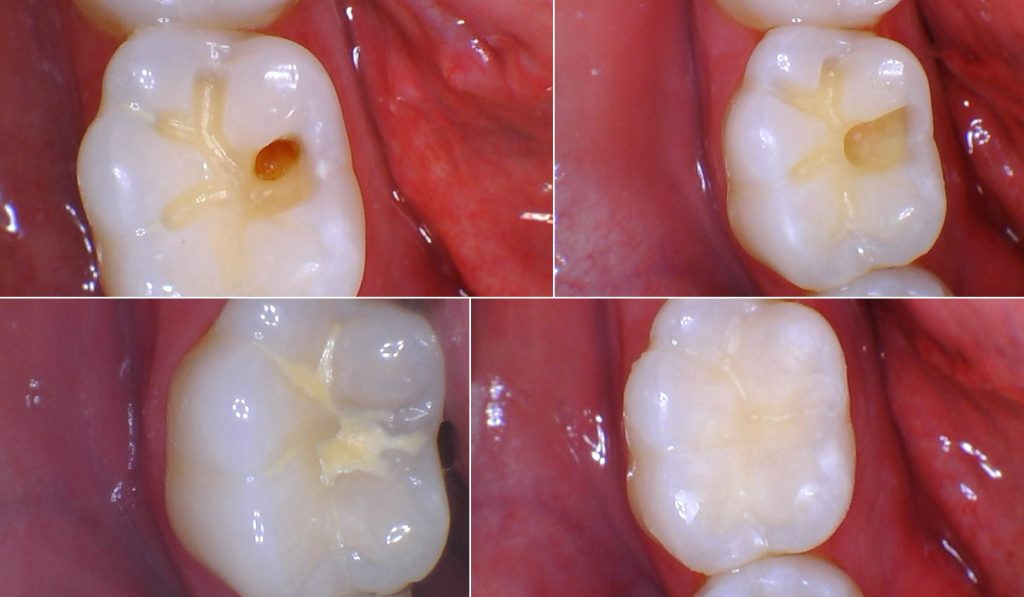
The first step is to use a very small, pointed, carbide bur and clean out the pits and fissures and widen them; this is called fissurotomy or enameloplasty. The surface of the tooth to be sealed is then air abraded with 50um Aluminum Oxide powder. This step cleans bacteria and other deposits off the enamel to be sealed. Phosphoric acid is used to etch the enamel and is rinsed off. The tooth is dried and isolated and a bonding resin is applied and air thinned.
Thin, flowable composite resin is placed in the prepared pits and fissures and hardened with a special curing light. Sometimes a slight adjustment to the bite is needed when placing a sealant this way due to the firmness of the material used. A sealant placed this way should last a very long time, possibly forever, and is much better at preventing tooth decay in the pits in fissures than a traditionally placed sealant.
The REALITY
There are downsides and challenges to the “Ideal Sealant” technique or PRR on children. First and foremost, it takes considerably more time to place the sealant and a young child may become restless. Additionally, children may not tolerate the “drilling” needed to prepare the tooth. You must
keep the tooth free from saliva and any contamination, which is difficult in a small mouth with an active tongue and saliva production.
Materials and labor also cost more for the “Ideal” sealant. Along with the addition of time for the procedure, only a dentist can do the fissurotomy. Many sealants are placed at programs at schools by Dental Hygienists in order to provide better access for children. Insurance reimbursement for sealants is very low and Insurance contracts do not allow a patient to choose a better method of doing a sealant. A dentist under contract with the insurance cannot even offer the service outside of the insurance without violating the contract.
The best suggestion is to seal teeth as soon as they erupt and as early as possible in children. Then, monitor the sealants over time and replace those that show signs of problems. As a teenager or adult, you can choose to remove the sealants and place Preventative Resin Restorations (PRR), on the back teeth for a more definitive “Ideal Sealant”.
If you have any questions, please contact our office!